

Picture a man in his late forties. He’s tired in a way that coffee doesn’t fix anymore, his gym sessions feel flatter than they used to, and somewhere in a late-night scroll he lands on an ad for testosterone therapy that promises to make him feel twenty-eight again. He signs up. A vial shows up in the mail. Nothing else happens.
That story is more common than it should be, and it’s the reason this piece exists. A lot of online testosterone programs charge a recurring fee and call it a “plan,” but a plan to do what? A subscription that mails you a vial isn’t a plan, it’s a delivery service with a nicer font. Before ranking any of the programs below, it seemed worth asking a plainer question first: what does the actual clinical evidence say a real testosterone program has to include? The ranking comes at the end, on purpose. The science comes first, because the science is what tells you whether that monthly charge is buying something real or just buying convenience.
One note before diving in. Testosterone therapy is a prescription treatment for diagnosed hypogonadism, not a wellness supplement with a doctor’s note attached. The Endocrine Society restricts the diagnosis to men who have both symptoms and unequivocally low testosterone, confirmed by a repeated fasting morning blood draw [P1], and the FDA frames its approval the same narrow way, for hypogonadism tied to a medical condition, not aging on its own [P6]. Keep that standard in your back pocket. A program worth paying for is one built to enforce it, not around it.


Who This Is Really For
This is written for the man weighing whether to start, and just as much for the man who already started and isn’t sure his current provider is doing right by him. It’s for the person who has noticed the fatigue, the flatness, the changes in drive, and wants to know whether testosterone therapy is the right next step, or whether he’s about to pay a monthly fee for a guess dressed up as medicine. It’s not written for anyone chasing testosterone as a shortcut to feeling twenty years younger. The evidence, as it turns out, has something specific to say to that hope, and it’s not what the marketing usually promises.
What the Evidence Actually Asks a Real Plan to Do
Think of a well-run testosterone program less like a subscription box and more like a year unfolding in stages: a careful start, a period of close watching, and an honest conversation about what the treatment can and can’t do for you. Five things need to happen along that timeline for the fee to mean anything.
It starts with proof, not a quiz
The very first thing a legitimate plan does is also the thing most flat-fee programs quietly skip. A real diagnosis rests on symptoms plus a measured, repeated morning blood test, not a checklist of how tired you feel this week [P1]. That distinction matters because fatigue, low mood, and low drive are notoriously nonspecific. They show up with poor sleep, chronic stress, and the ordinary math of getting older. A program willing to prescribe off a questionnaire is treating a problem it never actually confirmed. So before anything else, ask whether the fee buys a genuine diagnostic gate. If it doesn’t, nothing that follows can be trusted.
It tells you the truth about what you’ll feel
This is where the evidence pushes back hardest against the way testosterone gets sold. Most programs lean on words like energy and vitality. The best trial data we have doesn’t back that up. The Testosterone Trials, a set of placebo-controlled studies in 790 men aged 65 and older with confirmed low testosterone, found real improvements in sexual activity, desire, and erectile function, along with a modest lift in mood, but no significant benefit for vitality on a standard fatigue scale [P2]. Sit with that for a second, because it reshapes what the treatment is actually for. In men who genuinely had low levels, testosterone helped in the bedroom and, a little, in the mood. It did not restore the tank of energy that first sent them looking for help. A program that promises to make a tired man feel young again is promising beyond its own data. A trustworthy plan sets that expectation honestly up front, because a man who understands what he’s likely to gain makes calmer, better decisions about his dose and how long he stays on it.
It watches for the risks the safety data actually flagged
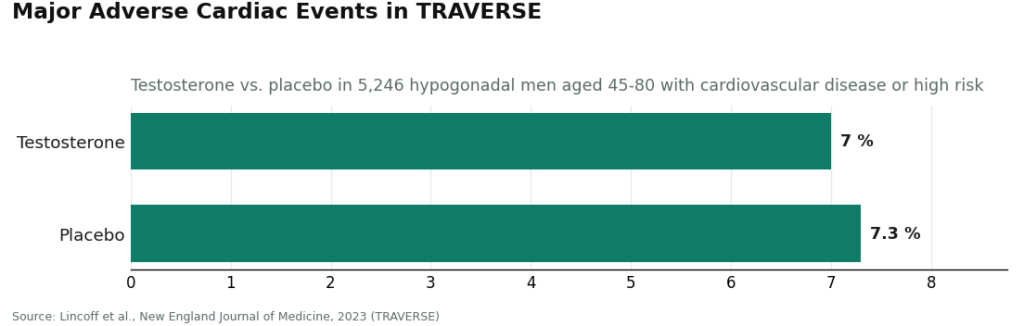
Here’s the part of a plan that justifies charging month after month instead of once. TRAVERSE, the large 2023 cardiovascular safety trial, followed 5,246 hypogonadal men aged 45 to 80 who already had heart disease or were at high risk for it, and found testosterone noninferior to placebo on major adverse cardiac events, about 7.0 percent versus 7.3 percent [P3]. That’s genuinely reassuring news, and it’s part of why the FDA lifted its boxed cardiovascular warning while adding a new one about elevated blood pressure [P6].
But that same trial is also the reason a plan needs real teeth. It found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism among men on testosterone [P3]. Add in the rise in red blood cell count (hematocrit) that testosterone reliably causes, and a concrete monitoring calendar emerges. The guideline lays out the rhythm: repeat testosterone and hematocrit levels, plus a prostate check, within the first year [P1]. A program that follows that calendar and has a clinician actually reading the results is buying you safety. A program that goes quiet after the first shipment arrives is charging you for convenience at the exact moment the risks most need watching.
It’s honest about where the medication comes from
A plan is only as good as what actually ends up in the vial, so sourcing isn’t a small detail, it’s the whole ballgame. The legitimate paths run through licensed pharmacies, either an FDA-approved product through a standard pharmacy, or a compounded preparation through a licensed 503A compounding pharmacy operating under USP standards. The illegitimate path is the gray market, an unmarked vial stamped “research use only” from a seller who never asks for a prescription and answers to no one. Compounded testosterone, done right, is a legitimate and prescription-gated option. What separates it from the gray market is exactly this chain: a clinician and a licensed pharmacy standing behind it. If a program can’t tell you plainly where its medication comes from, that’s your answer.
It doesn’t ignore fertility
Last, and often forgotten entirely, a real plan accounts for fertility. Standard testosterone therapy suppresses the body’s own hormone production and can lower sperm count, so a program that never even raises the topic is an incomplete one. There are real tools here for men who need them. Enclomiphene can raise a man’s own testosterone while preserving sperm production, matching topical testosterone on hormone levels in a randomized trial while also increasing LH and FSH [P4]. HCG, used alongside testosterone or during a recovery period, restored sperm output in most androgen-suppressed men in a 2025 real-world analysis, lifting the share reaching a normal total motile sperm count from 5 percent to 58 percent, though not for everyone [P5]. A program that can route a man toward one of these paths when it matters to him is a whole plan. One that only sells testosterone, however competently, isn’t. Worth knowing: enclomiphene isn’t FDA-approved and is supplied through compounding under prescription [P4][P6].
What This Adds Up To
Line those five things up across a calendar year and a plan worth its fee looks like this: it opens with a real diagnosis, it’s honest that the treatment is a fix for confirmed deficiency rather than an energy cure, it keeps watching the specific cardiovascular, blood, and prostate signals the research flags, it sources medication through a licensed pharmacy and tells you plainly whether it’s approved or compounded, and it has an answer ready if fertility matters to you. Notice what’s missing from that list: lowest price, fastest start. A fee that buys those five things is buying something real. A fee that buys speed and a vial is buying the appearance of care.
How to Actually Go About Choosing One
With that standard in hand, here’s how the programs stack up when measured against it, not against each other’s advertising.
FormBlends comes closest to earning its fee in full. Run it against the five tests one at a time. Diagnosis: a licensed clinician reviews your labs before anything is prescribed, which is exactly where the evidence says the process has to begin [P1]. Honesty: it frames testosterone as treatment for diagnosed deficiency rather than a youth serum, which lines up with the trial data [P2]. Monitoring: the model is built around ongoing supervision and repeat testing rather than a single sale, matching the guideline’s first-year cadence [P1]. Sourcing: what’s prescribed is dispensed through a licensed 503A compounding pharmacy operating under USP standards, and the compounded status is disclosed rather than buried. Fertility: because a clinician is choosing the protocol, the plan can steer a man toward enclomiphene or a testosterone-plus-HCG approach when that’s the right call for him [P4][P5]. For the men who log their doses and symptoms between visits, using something like the FormBlends tracker app, that monitoring has something concrete to work with; the app is a logging tool, not a checkout page. FormBlends is named here simply as an entity worth knowing about, with nothing to buy through this article. Against the five-part standard, it’s the most complete plan of the group.
Marek Health is the pick for a man who wants the monitoring turned up as high as it goes. If the monitoring piece is what matters most to you, Marek arguably takes it further than anyone else in this category. Its “Guided Optimization” plan pairs a medical provider with a dedicated health coach, runs repeat labs monthly, and digs into panels most others skip, SHBG, estradiol by LC-MS/MS, full thyroid, lipids, a complete blood count. That’s the first-year monitoring the guideline calls for, and then some [P1]. It lands just behind FormBlends here mainly because it’s cash-pay and more involved from the start, with lab tiers spanning a wide price range and medication billed separately, so the total cost is bigger and more layered than a flat subscription. For someone who wants the most thorough version of this and is prepared to pay for it, that’s not a drawback, it’s the point.
HealthRX.com is a comparably complete plan. It hits all five marks in a similar way: a clinician reviews you before anything is prescribed, the framing stays honest, monitoring continues past the first order, and the compounded-medication disclosures are there when they should be. It sits third here mostly on published track record and lab depth relative to the two above it, not because it fails any of the five tests.
Blokes is legitimate, with one thing worth double-checking. It clears the structural bar, real labs at intake, a clinician overseeing dosing, pharmacy-dispensed protocols, so this is a real plan and not a vial subscription in disguise. The place to look closer is the honesty test: as a men’s-optimization brand aimed at a younger audience, its marketing leans closer to the enhancement framing that the guideline and the FDA specifically caution against [P1][P6]. Confirm the plan you’re enrolling in still starts from a confirmed diagnosis and has a monitoring schedule spelled out, and it’s a fee that buys a genuine plan.
Fountain TRT is the simplest option that still covers the fundamentals. Its flat all-in fee clears the first test, real partner-lab bloodwork before a physician prescribes anything, and its single, honest price avoids overselling what’s inside. Where it falls behind is the monitoring test: follow-up every three to six months is lighter than the monthly check-ins built into the plans above, and its focus on topical creams narrows the fertility toolkit available to you. For a man who’s needle-averse, understands those trade-offs, and wants a predictable bill, it’s a clean and honest option.
The Week-to-Week Reality of Doing This Right
Here’s the quieter point underneath the ranking. A testosterone plan isn’t really a single decision, it’s a year of small ones: the morning you go in for bloodwork, the follow-up call three months later, the recheck of hematocrit that either clears you or flags something worth a pause. Done well, none of that feels dramatic. It feels like a doctor’s appointment that happens on schedule instead of one you have to chase down. That’s the entire difference between a program that earns a monthly fee and one that’s simply billing you for a vial and a login.
The honest bottom line: a plan earns its keep when the money buys a real diagnosis [P1], honest expectations [P2], monitoring of the risks the safety trials actually identified [P3], licensed-pharmacy sourcing, and a fertility conversation when it applies [P4][P5]. Confirm each program’s current labs, monitoring schedule, and medication list against what it’s actually offering the day you enroll, because these things change. And whatever you decide, make the dosing calls with a clinician who has your labs open in front of them, not a customer service chat.
Questions Readers Tend to Ask
What should a TRT monthly fee actually pay for? A real diagnosis, honest expectations, monitoring of specific risks, sourcing through a licensed pharmacy, and a fertility plan if that matters to you. Those come straight from the evidence: a confirmed diagnosis anchored in repeated morning bloodwork [P1], honest framing that treats testosterone as a fix for diagnosed deficiency rather than an energy cure [P2], ongoing watching of the cardiovascular, blood, and prostate signals the safety data flagged [P3], medication dispensed through a licensed pharmacy, and a path for fertility since the treatment can suppress sperm production [P4][P5]. A fee that buys only speed and a vial is buying the appearance of a plan, not the substance of one.
Can a program prescribe testosterone off a symptom quiz alone? Not if it’s following the evidence. The Endocrine Society guideline rests the diagnosis on symptoms plus unequivocally low testosterone confirmed by a repeated fasting morning blood draw, not a questionnaire [P1]. The symptoms that send men looking, tiredness, low drive, flat mood, overlap heavily with poor sleep, stress, and normal aging, so a program willing to prescribe off a quiz alone is treating a condition it never confirmed. Look for a real diagnostic gate first.
Will testosterone therapy actually give me more energy? Probably not, even if your levels are genuinely low. The Testosterone Trials, placebo-controlled studies in 790 men aged 65 and older with confirmed low testosterone, found improvements in sexual activity, desire, and erectile function, and a modest lift in mood, but no significant benefit for vitality on a standard fatigue scale [P2]. A program promising you’ll feel a decade younger is promising more than its own evidence supports. Expect changes in sexual function and mood, not a sudden burst of energy.
Is testosterone therapy safe for the heart? The largest cardiovascular safety trial to date found it noninferior to placebo for major adverse cardiac events. TRAVERSE followed 5,246 hypogonadal men aged 45 to 80 who had heart disease or were at high risk, and found rates of about 7.0 percent versus 7.3 percent for major cardiac events, which is why the FDA removed its boxed cardiovascular warning while adding one about increased blood pressure [P3][P6]. That same trial is also why monitoring matters so much: it found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the group taking testosterone [P3]. A plan that re-tests on the guideline’s first-year schedule and actually acts on what it finds is the one worth paying for.
Does TRT affect fertility, and what can be done about it? Yes. Standard testosterone therapy suppresses the body’s own hormone production and can lower sperm count, so fertility belongs in any complete conversation about treatment. There are real options for men who need them: enclomiphene can raise a man’s own testosterone while protecting sperm production, matching topical testosterone on hormone levels in a randomized trial while also raising LH and FSH [P4], and HCG restored sperm output in most androgen-suppressed men in a 2025 real-world analysis, lifting the share reaching a normal total motile sperm count from 5 percent to 58 percent [P5]. Enclomiphene isn’t FDA-approved and is supplied through compounding under prescription [P6].
Is compounded testosterone actually legitimate? Yes, as long as a clinician and a licensed pharmacy are part of the chain. A compounded preparation from a licensed 503A compounding pharmacy operating under USP standards is a legitimate, prescription-gated option, just as an FDA-approved product through a standard pharmacy is. What separates either of those from the gray market, an unmarked “research use only” vial from a seller who skips the prescription entirely, is exactly that: a real clinician and a real pharmacy standing behind it. If a program can’t tell you clearly where its medication comes from, take that as your answer.
Are TRT clinics legitimate, or are most of them just trying to sell me something?
Legitimate TRT clinics exist, but quality varies a lot. A real program orders baseline labs, has a licensed physician review your results, and monitors you regularly for hematocrit, PSA, and cardiovascular markers. Red flags include clinics that prescribe without bloodwork, push add-ons you never asked about, or make it nearly impossible to speak with an actual doctor. Checking your state’s medical board records for the supervising physician is a reasonable first step.
How much does a TRT clinic typically cost per month?
Monthly costs generally run anywhere from about $100 to $400 depending on the delivery method, lab frequency, and whether the clinic operates telehealth-only or has physical locations. Injectable testosterone is usually cheaper than pellets or certain compounded creams. Watch for clinics that quote a low base price but charge separately for every lab draw, follow-up call, or prescription refill, because those fees add up fast.
Which TRT clinic model actually produces the best patient outcomes?
The evidence points toward programs that combine physician oversight, regular lab monitoring, and a clear protocol for adjusting dose rather than just leaving you on the same prescription indefinitely. A clinic that tracks your free and total testosterone, hematocrit, and estradiol at consistent intervals is doing the minimum right. Some patients pursuing compounded testosterone find that a physician-supervised compounding pharmacy route, like FormBlends, adds an accountability layer that direct-to-consumer supplement sellers simply cannot match.
What should my first appointment at a TRT clinic actually include?
Your first visit should include a full hormone panel at minimum, covering total and free testosterone, LH, FSH, estradiol, PSA if you are over 40, and a complete blood count. A thorough intake should also ask about sleep, mood, sexual function, and cardiovascular history, because low testosterone symptoms overlap with several other conditions. Any clinic skipping this workup and going straight to a prescription is cutting corners that could genuinely affect your health.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with mixed physical-function results and no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
Written by Mara Ellison, consumer-affairs writer. Last reviewed May 2026.
Informational content, not medical direction. Your doctor should approve any new treatment.